A 42 year old man presents with shortness of breath on exertion for three weeks. He was initially diagnosed with asthma by his GP, and had some improvement with salbutamol and fluticasone. However, in the past week or so he feels his puffers are no longer helping. He felt “warm” at home (no documented fever), and his co-worker was recently diagnosed with “double pneumonia.” He is wondering if he needs antibiotics. He has had a mild non-productive cough, and denies chest pain, hemoptysis, and orthopnea/PND.
Past medical history
Remarkable only for mild hypertension. He is on no other medications, and is a nonsmoker.
On exam
Looks well with no increased work of breathing. Vitals: T36.1, HR 108, RR 18, BP 128/66, Sats 96% RA
Heart sounds are normal but there is a mild systolic murmur best heard at the apex. Chest is clear, and the rest of the exam is benign. He has no pedal edema, calf swelling, or calf tenderness.
Investigations
High-sensitivity troponin of 35 (no previous, repeat 32). All other labs are normal.
EKG shows LVH with nonspecific T-wave abnormalities.
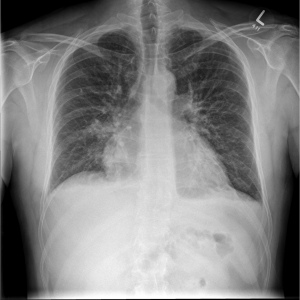
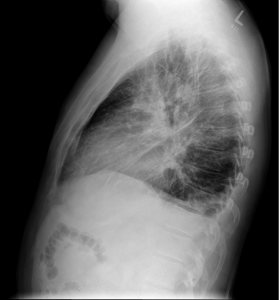
CXR
Under-expanded lungs (which likely accounts for the apparent cardiomegaly/prominence of lung markings), and a focal air space shadowing at the right base (also seen on lateral film) in keeping with infection. Possibly a small amount of pleural fluid.
What would you do? Send him home with antibiotics for pneumonia? Perhaps outpatient f/u for his mild troponin elevation? What about his tachycardia? Is it related to the infectious process? Too much salbutamol? Does he have something more sinister like a PE?
This is where bedside ultrasound can help!
Click to continue case