


THE CASE
A 63 year-old lady fell outdoors after she was pulled over by her very bad dog. Apparently there was a squirrel.
She fell on her right side and her efforts to save her Starbucks landed her directly on her elbow.
Thanks to 4-point limb contact the dog stayed upright, the squirrel is still at large.
INITIAL ASSESSMENT
Swollen, tender right elbow, held adducted in flexion.
Tender to posterior elbow, over olecranon.
ROM from 60° – 120°, limited by pain.
No pain with pronation-supination.
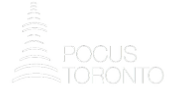
XRAY
To save you from squinting – the radiology read was:
No fracture seen, but highly suspicious for fracture based on soft tissue findings.
See Grayson for an excellent review of Elbow Radiography1.
THE SAIL SIGN
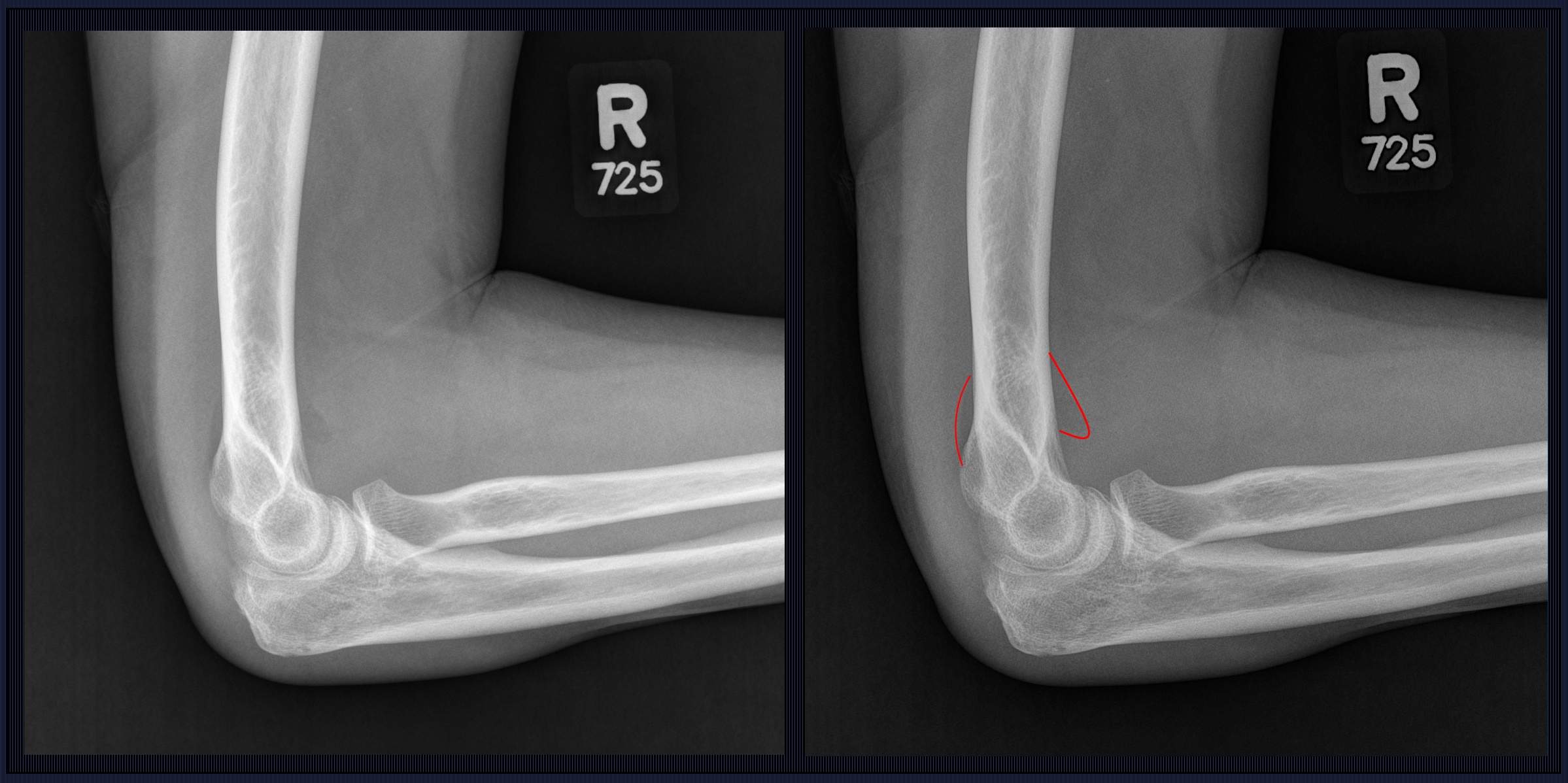
The ‘sail sign’ refers to the posterior fat pad visible on the lateral xray.
Hemarthrosis displaces the fat pad superiorly causing the triceps tendon to tent slightly.
Keep in mind that this sign is not specific to traumatic effusions so if there is doubt
comparison should be made with the contralateral side.
In the case of a traumatic effusion, the culprit fractures are:2
Radial Head or Neck – 86%
Olecranon – 7 %
Lateral Epicondyle – 7%
Playing the odds, this is a radial head or neck fracture.
Clinically the patient was most uncomfortable with flexion/ extension, and minimal pain
with supination pronation, not in keeping with a break in the proximal radius.
HOW ABOUT POCUS?
Assessment of the elbow with US has been well described. A recently published prospective study in AJEM suggested that PoCUS was 97% sensitive and 88% specific for the diagnosis of fractures of the bones of the elbow 3.
In a 2015 study PoCUS correctly classified 83% of radial neck fractures and 65% of radial head fractures among patients with a posterior fat pad but no fracture visible on plain radiograph 4.
Since the humerus sits on a cavity formed by the trochlear notch of the olecranon, all olecranon fractures are intra-articular 5. This means that an olecranon fracture can result in a ‘sail sign’ in the absence of radial pathology.
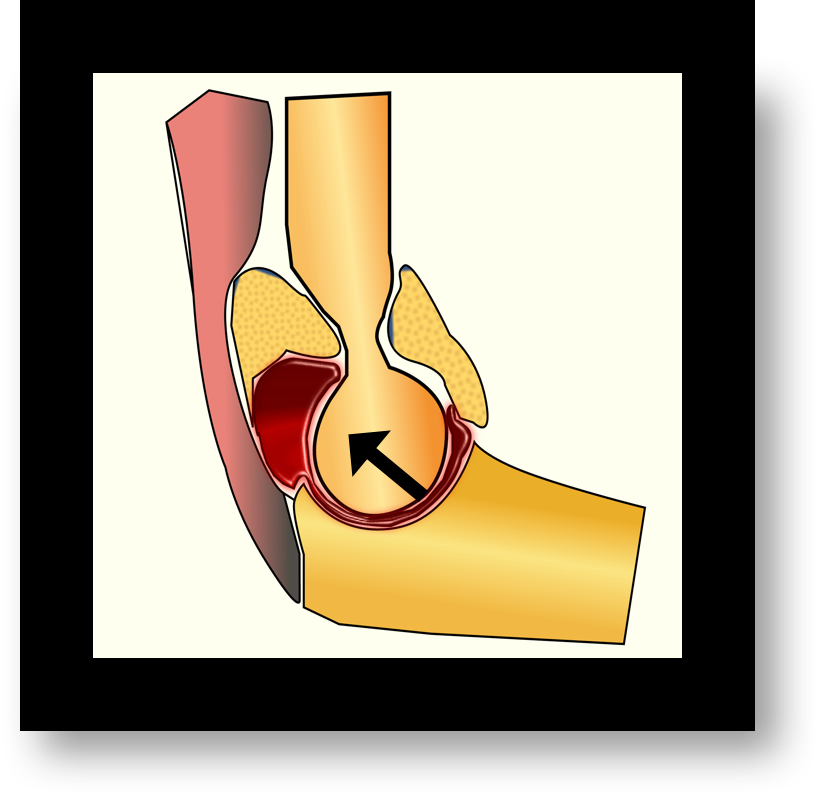
THE SCAN
Start by assessing the posterior humerus in a longitudinal plane and look for joint effusion.
Here is the image again with a markup for reference:

Next rotate 90 degrees. Here is the short axis view of the same patient.
![]()
You can see the joint space and effusion between the humeral epicondyles.
Next scan the olecranon process of the ulna. Follow the curve and assess for cortical discontinuity.
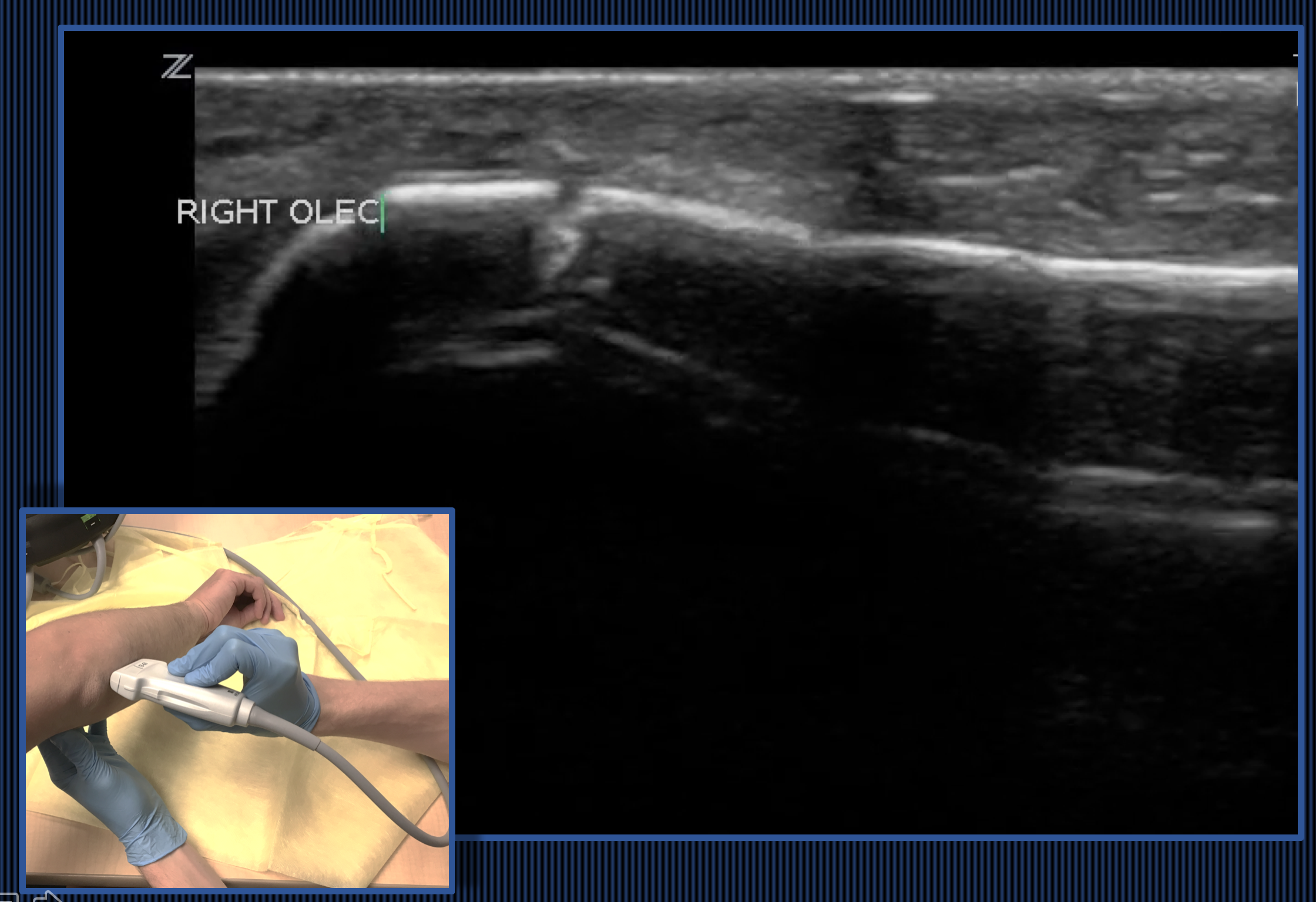
Again, rotate 90 degrees and interrogate in transverse. Here is a clip:
Note the break in the cortex. This fracture was invisible to plain radiograph
Finally place the probe longitudinally along the axis of the proximal radius to view the radial head and neck.
Having the patient supinate pronate slowly can help interrogate the radial head.
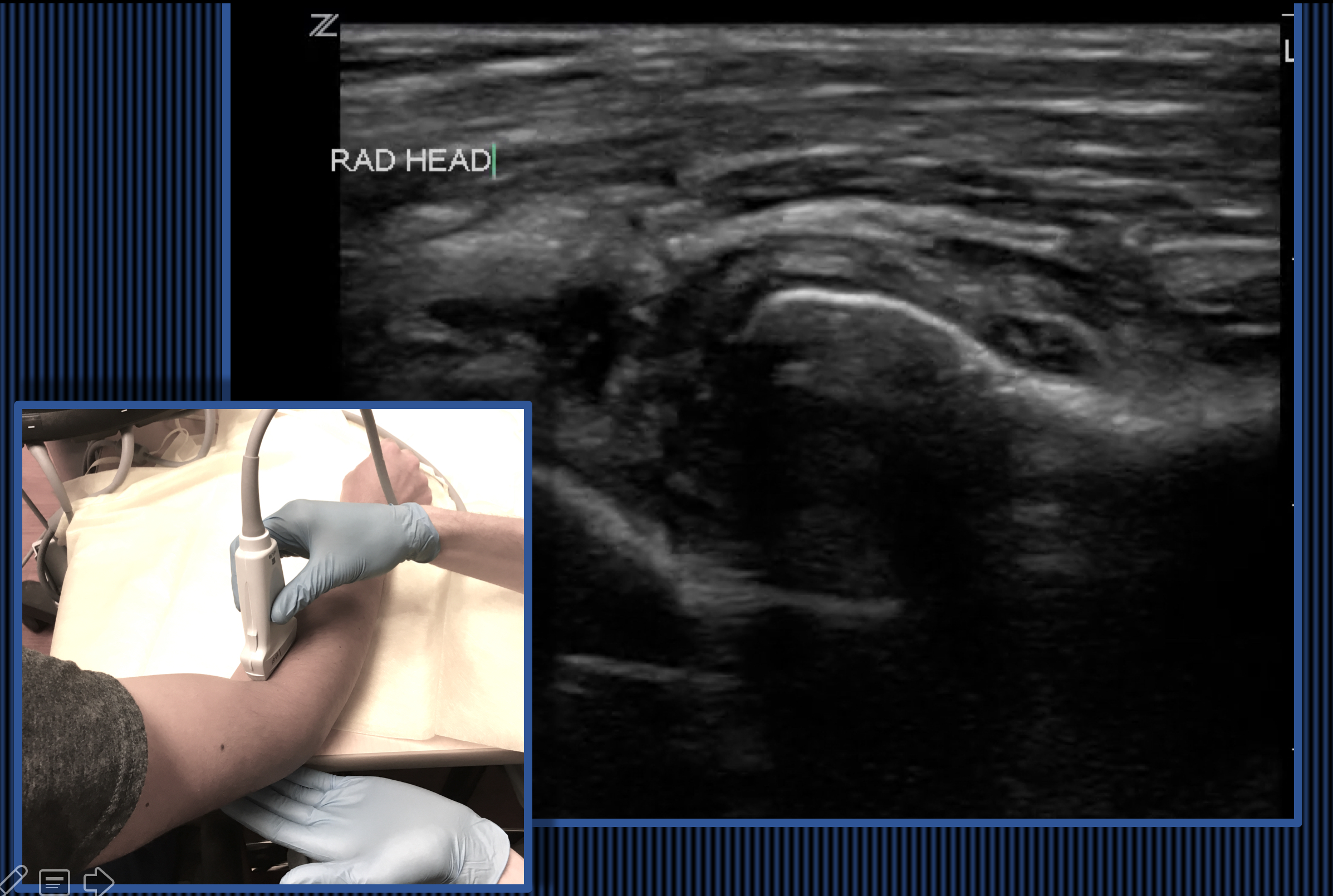
Repeat in short axis and watch the spin…
![]()
BACK TO THE CASE
As the importance of maintaining mobility following radial head fractures becomes increasingly apparent, distinguishing an olecranon fracture (which always requires immobilization with a posterior slab) and a radial head fracture may become more significant.
The olecranon is the site of insertion of the triceps, contraction of which can lead to a displacing force. This can lead to elbow instability through the posterior displacement of the distal humerus.
HOW SHOULD ELBOW POCUS BE USED?
Sort out occult radial head vs olecranon vs distal humerus and reduce CT use.
In our ED, this is likely not of major consequence as we have the luxury of easily accessible advanced imaging and short-term orthopedic follow up, but this US still prompted a change in management.
Replace the elbow xray as initial screen – especially in kids.
One pediatric study showed utility in using POCUS assessment of hemarthrosis/posterior fat pad as a “FAST exam for the traumatized elbow” to rule out elbow fractures without radiation.
Rule out open fracture.
We had another patient with a very similar story several days later. She had fallen and sustained a puncture to her right elbow but had not sought medical attention. She complained of increasing pain and some purulent discharge from the wound. Cellulitis? Open fracture? Septic arthritis? POCUS lets you check for an effusion and inspect for occult fractures.
Like many things in PoCUS, assessment of elbow injuries with plain radiograph will likely remain standard of care for the foreseeable future.
Notwithstanding, this tool is a helpful adjunct that may outperform plain radiography for certain pathology,
… and if you find no other use for it… watch the radius spin… it’s strangely fun.
References
- Grayason DE. The Elbow: Radiographic Imaging Pearls and Pitfalls. Seminars in Roentgenology. 2005.
- O’Dwyer H, O’Sullivan P, Fitzgerald D, et al. The fat pad sign following elbow trauma in adults: it’s usefulness and reliability in suspecting occult fractures. Journal of Computer Assisted Tomography. 2004. 28(4):562-65.
- Avci M, Kozaci N, Beydilli I, Yilmaz F, Eden AO, Turhan S. The comparison of bedside point-of-care ultrasound and CT in elbow injuries. AJEM. 2016. 34:2186-90.
- Pavic R, Margetic P, Hnatesen D. Diagnosis of occult radial head and neck fractures in adults. Injury. 2015. 46S:119-124.
- Avci M, Kozaci N, Beydilli I, Yilmaz F, Eden AO, Turhan S. The comparison of bedside point-of-care ultrasound and CT in elbow injuries. AJEM. 2016. 34:2186-90.
- Wiegand L, Bernstein J, Ahn J. Fractures in Brief: Olecranon fractures. Clinical Orthopedics and related research. 2012. 470:3637-41.
- Tsung JW, Blaivas M. Rapid screening for the posterior fat pad sign in suspected pediatric elbow fracures using point-of-care ultrasound: a “FAST exam” for the traumatized elbow. Critical Ultrasound Journal . 2010.

- Needle Guidance for Procedural Ultrasound - April 9, 2017
- POCUS for Elbow Injuries - February 17, 2017
- Where the Right Upper Quadrant Goes Wrong … pearls and pitfalls in the FAST exam - January 27, 2017
2 Comments
As good as always!
Conclusion: In conclusion, POCUS was shown to be successfully applied in the diagnosis and management of elbow injuries, in which direct radiography was inefficient and CT scans were required.